.png)
.png)

BC EMALB Practical Examination Guidelines
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial Examination Guidelines")
The Canadian Red Cross, BC Ambulance Service and BC Emergency Medical Assistant's Licensing Branch follow the National Occupational Competency Profile (NOCP) for most EMR skills, as endorsed by the Paramedic Association of Canada (PAC). EMALB, the agency responsible for Licensing evaluations in British Columbia, has additional, sometimes contradictory requirements to successfully complete their practical scenario examinations. These requirements are outlined in the EMALB British Columbia Provincial Examination Guidelines booklet. Whenever the BC EMALB Examination Guidelines contradict or supplement the information provided in the Canadian Red Cross Emergency Care for Professional Responders text book, the EMALB Examination Guidelines take precedence and overrule any other interpretations.
The Emergency Medical Assistants Licensing Board British Columbia Provincial Examination Guidelines for Primary Care Paramedics and Emergency Medical Responders is produced and updated by the BC EMALB team of medical professionals and advisors. The purpose of the Guidelines document is provide insight and consistency for Emergency Medical Responder and Primary Care Paramedic course students preparing for their EMALB practical scenario evaluations.
It is important to note that the BC EMALB Provincial Examination Guidelines include skills and protocols at the Primary Care Paramedic (PCP) level as well as the Emergency Medical Responder (EMR) level. Take care to differentiate the PCP only components when reviewing the Examination Guidelines for purposes of preparing for practical scenario Licensing evaluations at the Emergency Medical Responder level. It would be inappropriate to implement PCP level skills and decisions during EMR examinations, and this would likely result in an unsuccessful result.
For the most part, the EMALB Examination Guidelines for EMR skills follow the same protocols, principles and processes as those outlined by the Canadian Red Cross and PAC NOCP. However, there are a few specific Examination Guidelines which differ slightly from the National PAC NOCP, which means you need to be aware of them for BC EMALB EMR Licensing purposes. The EMALB British Columbia Provincial Examination Guidelines that are particularly relevant to Emergency Medical Responders in British Columbia are listed in detail below, on this page.
These specific Examination Guidelines include:
Updates to the EMALB Examination Guidelines
.jpg "Updates to the Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines")
BC EMALB does update their examination guidelines, and the corresponding treatment protocols required to meet Licensing requirements, on a regular basis without advance notice. It's definitely a good idea to revisit and review the most current version of the Examination Guidelines as you prepare for your EMALB Emergency Medical Responder or Primary Care Paramedic practical scenario exams.
The cover page of the Examination Guidelines booklet states that these guidelines were produced by the Ministry of Health in 2019. However the bottom right footer on the interior pages shows the date of the most recently published version (ie..."Current July 27, 2022"). Checking the footer date can help you determine if any significant changes may have been implemented in the time since your most recent certification training.
If you completed your most recent Emergency Medical Responder certification training course prior to the updates listed below, you should definitely revisit these skills and topics before completing your upcoming BC EMALB written and practical examinations. Many of these topics are covered in more detail throughout Medi-Pro's EMR Study Guide, EMR Cheat Sheet, and other online resources on Medi-Pro's website.
Recent EMR level updates to the EMALB Examination Guidelines:
July 27, 2022
March 16, 2022
NEXUS Spinal Motion Restriction
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for Spinal Motion Restriction and Modified NEXUS")
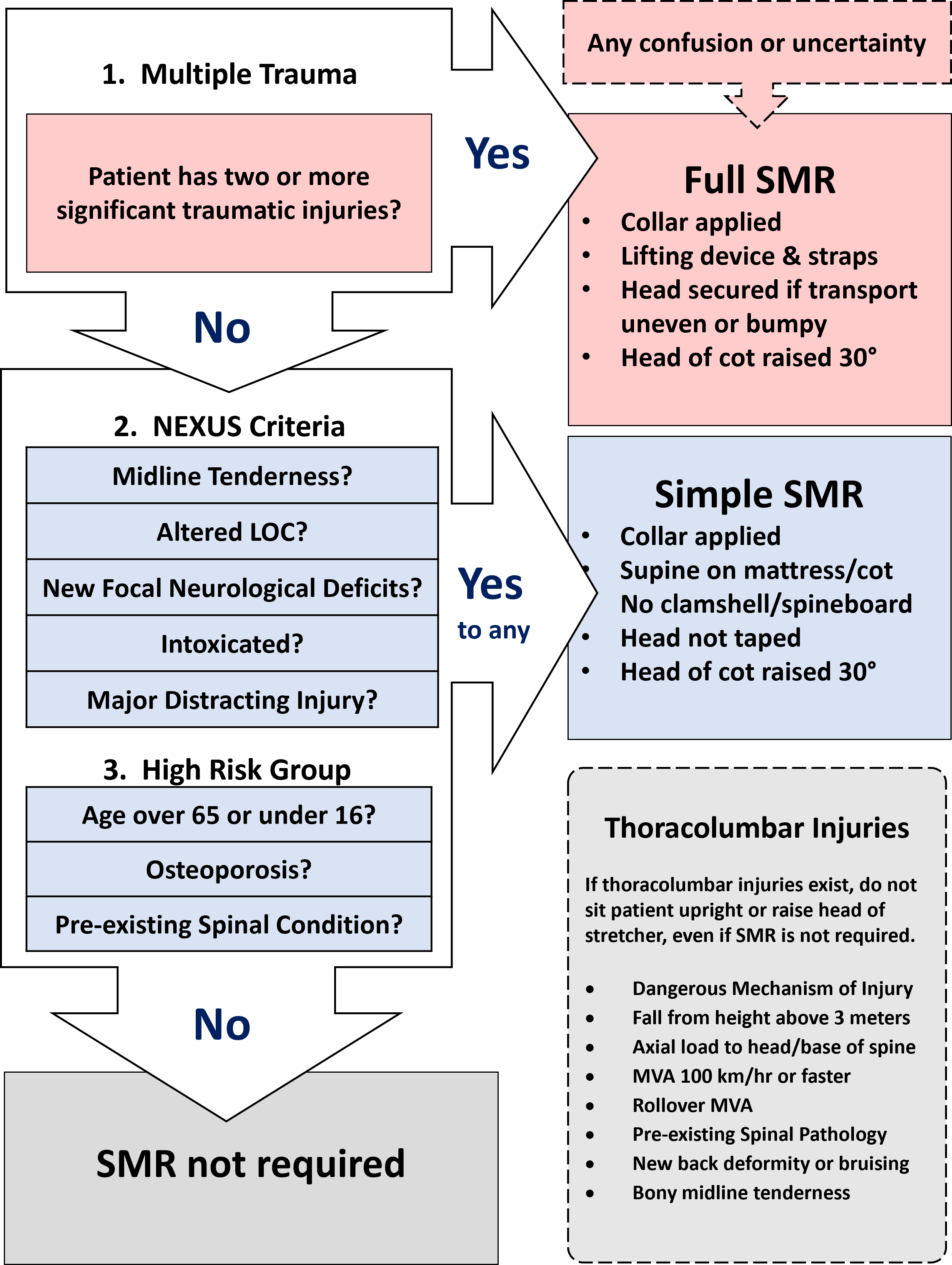
A significant portion of your EMR training course involves learning and practicing the prinicples of Spinal Motion Restriction (SMR), the Canadian C-Spine Rules, and the National Emergency X-Radiological Utilization Study (NEXUS) protocols which replaced the older Spinal Immobilization approach. The new SMR guidelines and accompanying modified NEXUS protocols adopted by BC EMALB provide paramedics with more options and flexibility to provide patient care when spinal cord injury is suspected, but the complex decision matrix requires memorization and practice.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
NEXUS SMR Decision Matrix for Injuries with Spinal Mechanism
Determining Cardiac Arrest for Hypothermic Patients
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for assessing the pulse on a hypothermic patient.")
As Hypothermia progresses from mild, to moderate and eventually to the severe category, the body's metabolic process can slow to an almost imperceptible rate. This can make it challenging to definitively determine the presence or absence of a carotid pule, prior to begining CPR-AED protocols when the patient is not breathing and appears otherwise lifeless. The heart could still be beating, just at a rate and strength that makes it difficult to detect. For this reason, you should take a bit of extra time and care when performing your Primary Assessment, particularly the Airway, Breathing, and Circulation check if hypothermia is known or suspected to be a factor.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
AED Shock Limits for Hypothermic Patients
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for performing CPR and using an AED on a Hypothermic patient.")
When performing Basic Life Support level CPR and following Automated External Defibrillation (AED) protocols on a patient who is significantly/severely hypothermic, the AED may become less effective than normal. At a certain point, the time spent interrupting compressions to allow the AED to analyze the heart rhythm for Ventricular Tachycardia or Ventricular Fibrillation may hamper rescuscitation efforts, with a dimishing chance of positive outcomes. The relatively small chance that the AED shock will result in return of spontaneous circulation (ROSC) is no longer sufficient to justify the loss of coronary perfusion pressure (CPP) during pauses in compressions.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Pediatric Pulse Oximetry
The use and interpretation of a finger-tip pulse oximeter to measure a peripheral capillary oxygen saturation (SpO2) can provide valuable information about a patient's current condition, as well as benchmarks to determine if the patient's condition is improving or declining overall. As with any electronic device, there are limitations to the accuracy of pulse oximters, and certain conditions can compromise the accuracy of the data displayed. Sickle cell anemias, carbon monoxide poisoning, poor peripheral perfusion, and dirty/painted fingernails are examples of conditions which can cause a pulse oximeter to malfunction. When rescuers utilize a pulse oximeter it is important to rely on all the data available and to treat the patient appropriately to their overall condition, not just the readings of a single device.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Realignment of Grossly Deformed Limbs
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for treating limb threatening injuries and realigning grossly deformed extremities.")
The term "Gross Deformity" refers to a fracture or dislocation which, in addition to causing the pain and surrounding tissue damage typically associated with an injury of this type, has distorted the limb or extremity far beyond its normal anatomical position. This can cause other complications such as a lack of circulation distal to to the injury, which creates an urgent limb-threatening injury, and can render patient packaging and transport impractical or even impossible.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Sager Traction Splint
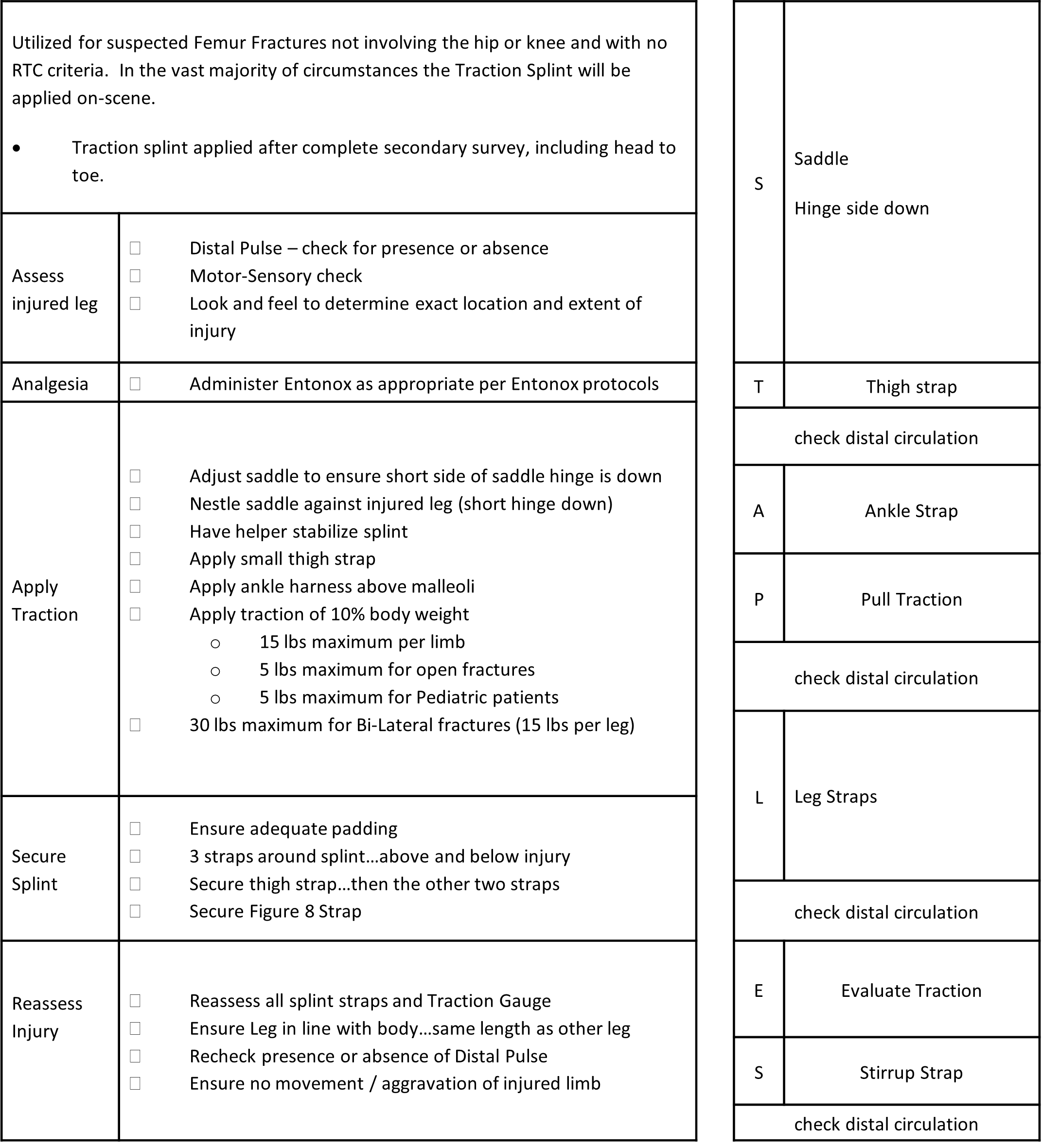
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for application of a Sager Traction Splint for patients with mid-third femur fractures.")
When properly applied, a traction splint can alleviate much of the pain from a femur fracture as well as preventing further interal tissue and blood vessel trauma by holding the fractured bone ends from grating against or sliding further alongside each other. The Sager traction splint is preferred by BCEHS and will be provided during EMALB Licensing evaluations, so examination participants must be proficient with this specific brand and EMALB's specifications for it's application. Optimal patient care when utilizing a SAGER Traction Splint also involves careful stabilization of the injury throughout application, judicious placement of securing straps and adequate padding to ensure there are no hot spots or excessive movement on the affected leg. Transport of a patient wearing a traction splint will usually involve placement of a Robertson Orthopedic Stretcher (Clamshell) under the patient prior to lifting onto the cot.
What the EMALB Examination Guidelines say:
Traction Splint Indications
Procedure
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Sager Traction Splint Mnemonic (STAPLES)
Treatment of Open Chest Wounds (Pneumothorax)
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for utilizing a Vented Occlusive Dressing on a sucking chest wound.")
Open chest wounds, also commonly referred to as sucking chest wounds, can indicate and contribute to an immediately life-threatening condition known as Tension-Pneumothorax. Essentially, the air normally moved in and out of the patient's lungs during respiration escapes through the ruptured thoracic tissues and accumulate in the thoracic cavity. Atomospheric air may also contribute to this accumulation if air enters into the cavity through the external wounds. The cumulative pressure of air trapped between the chest wall and internal organs can push and squeeze those organs in a manner that prevents their normal function. Most immediately this can affect the patient's ability to breathe and eventually cause cardiac failure.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Treatment of Burn Injuries
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for cooling burn injuries.")
Burn injuries can continue to cause additional pain and tissue damage even after the source of heat that originally created the burns has been removed. This is partly due to heat from the initial burn becoming trapped in the deep tissue layers surrounding the injured area, and continuing to inflame those tissues. For this reason, it is important to initiate cooling of burn injuries as soon as possible, so long as this does not distract you from dealing with other more crucial priorities. Cooling of burns, most often with sterile saline solution, may be initiated on-scene then continued while enroute to definitive medical care if life-threatening conditions put the patient into the urgent transport category.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Assessment of Stroke & TIA
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for assessing Stroke using the FAST VAN tool.")
When a blood clot, embolism, plaque or aneurysm prevents adequate blood flow to the brain, a part of the brain tissue can starve or die, causing a stroke. In some cases the blood flow may resume before permanent damage occurs, which is commonly referred to as a Transient Ischemic Attack (TIA). The longer the blood flow is disrupted the more brain tissue dies and the more dramatic and permanent the damage becomes. As the left side of the brain controls the right side of the body, and the right side of the brain controls the left side of the body, the physical effects/deficits created by the stroke are usually seen on the opposite side of the affected brain. Other than early recognition of the signs and symptoms of a potential Stroke, including sudden headache, one-sided weakness/paralysis, dizziness, confusion and slurred speech, there is very little that rescuers can do in the field to prevent ongoing brain tissue ischemia. The sooner a Stroke patient is transported to definitive medical care, the less brain function they will lose and the greater their chances of survival and recovery.
What the EMALB Examination Guidelines say:
FAST-VAN Pre-Hospital Stroke Tool
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Which Medications Licensed Emergency Medical Responders are Authorized to Administer in BC
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for Administration of Medications.")
The ability to administer medications to patients is a critical part of delivering emergency medical care, and carrys a correspondingly significant set of responsibilities. Licensed Emergency Medical Responders in BC are not authorized to provide all medications in all circumstances, and in many circumstances it is harmful to provide or assist with the wrong medication. Distinguishing between medications which can be administered, medications that can be assisted with, and medications which are contraindicated requires a strong understanding of pharmacology and continuous, ongoing review of current medication guidelines.
What the EMALB Examination Guidelines say:
BCEHS and the EMALB restrict licensed Emergency Medical Responders to Administering only specific medications. As an Emergency Medical Responder holding a BC EMALB License, you are authorized to carry administer the following medications, while employed in your duties as an EMR:
*Naloxone administration is not currently included in the baseline scope of practice for a licensed Emergency Medical Responder, but specific emergency response agencies in BC have special permission from BCEHS for their medical responders to carry and administer Naloxone, to mitigate the ongoing opioid overdose crisis. If the agency you work for, in your capacity as a licensed EMR/FR has this agreement in place you will receive agency specific training and then be authorized to carry and administer Naloxone as part of your medical response duties.
What this means for Emergency Medical Responders in BC:
Licensed Emergency Medical Responders in BC will Administer Oxygen, Glucogel, Nitroglycerin, ASA, Entonox and Naloxone* to patients when appropriate and in accordance with the specific protocol, indications and contraindications relevant to that particular medication.
Medication Administration Protocols
Medication Indications & Contraindications
Medication Cautions
Vital Signs Prior to Administration
Assisting with Medications
6 "Rights" of Medication
The 6 Rights of Medication are a memonic device to aid medical responders in systematically ensuring that assisting a patient with their medication is likely to be beneficial and unlikely to be harmful. If an EMALB Licensed medical responder is going to actually "Administer" medication, the specific protocols, indications, contraindications and cautions should be followed rather than the 6 Rights.
EMALB Licensed Emergency Medical Responders may routinely utilize the 6 Rights mnemonic to Assist patients with (but not Administer) commonly prescribed medications which can have acutely beneficial effects such as an EPI-Pen which delivers Epinephrine, and Asthma Inhalers which deliver Salbutamol/Albutrol.
Glucogel for Unresponsive Patients
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for Administration of Glucogel to a Hypoglycemic patient.")
For patients with confirmed Hypoglycemia, which in BC is considered a measured capillary blood glucose level (capBgl) below 4 mmoL/l, quickly raising their blood sugar levels can alleviate immediately life-threatening conditions including the associated decreased levels of consciousness. Glucose Gel (Glucogel) can be administered orally and alleviate hypoglycemia with little risk of negative effects or drug interactions, however there is a risk that the patient may choke on the gel if they are not completely responsive at the time of administration.
What the EMALB Examination Guidelines say:
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Administration of Nitroglycerin to Patients with or without a Prescription
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for Administration of Nitroglycerin to a patient with cardiac chest pains.")
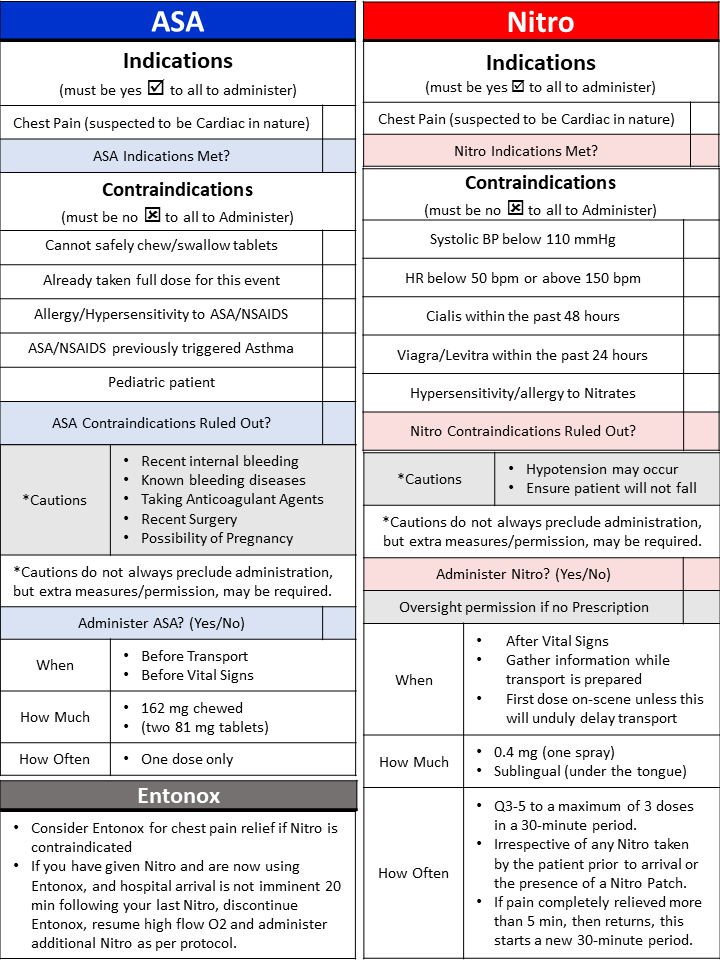
Nitroglycerin spray is a vasodilator, which means that the correct dose at the correct time can temporarily and partially alleviate the symptoms of acute myocardial infarction (AMI). The vasodilation that accompanies a dose of nitro can widen coronary arteries and leave more room for blood to flow past a blockage. Nitroglycerin can also create a dramatic drop in blood pressure, which can itself cause negative patient outcomes if not carefully monitored and mitigated. Administration of Nitro spray, whether to a patient with a previous Nitro prescription or to a patient with no previous prescription, requires strong familiarity with and stringent adherence to the associated protocols surrounding indications, contraindications, cautions, doeseage and frequency.
What the EMALB Examination Guidelines say:
Nitro Indications
Nitro Contraindications
Nitro Protocol
Contradictory information in the Emergency Care for Professional Responders text book:
What this means for Emergency Medical Responders in BC:
Administration of Acetylsalicylic Acid (ASA) before Vital Signs
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for Administration of Acetylsalicylic Acid (ASA) to a patient with cardiac chest pains.")
Acetylsalicylic Acid (ASA), also commonly referred to as Aspirin is both a platelet inhibitor and an anti-inflammatory. These properties can make ASA an extremely important and effective medication for patients experiencing acute myocardial infarction (AMI), as the platelet inhibitor effects prevent blood clots in the corornary artery from growing larger and the anti-inflammatory effects prevent the walls of the coronary ateries from becoming swollen and closing in on existing blockages. Because the positive effects of ASA during an AMI are so pronounced and time sensitive, it is the only only medication which can be administered without first collecting a complete set of Vital Signs.
What the EMALB Examination Guidelines say:
ASA Indications
ASA Contraindications
ASA Cautions
ASA Protocol
What this means for Emergency Medical Responders in BC:
Administration of Nitrous Oxide (Entonox)
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for Administration of Nitrous Oxide (Entonox) to a patient experiencing significant pain or discomfort.")
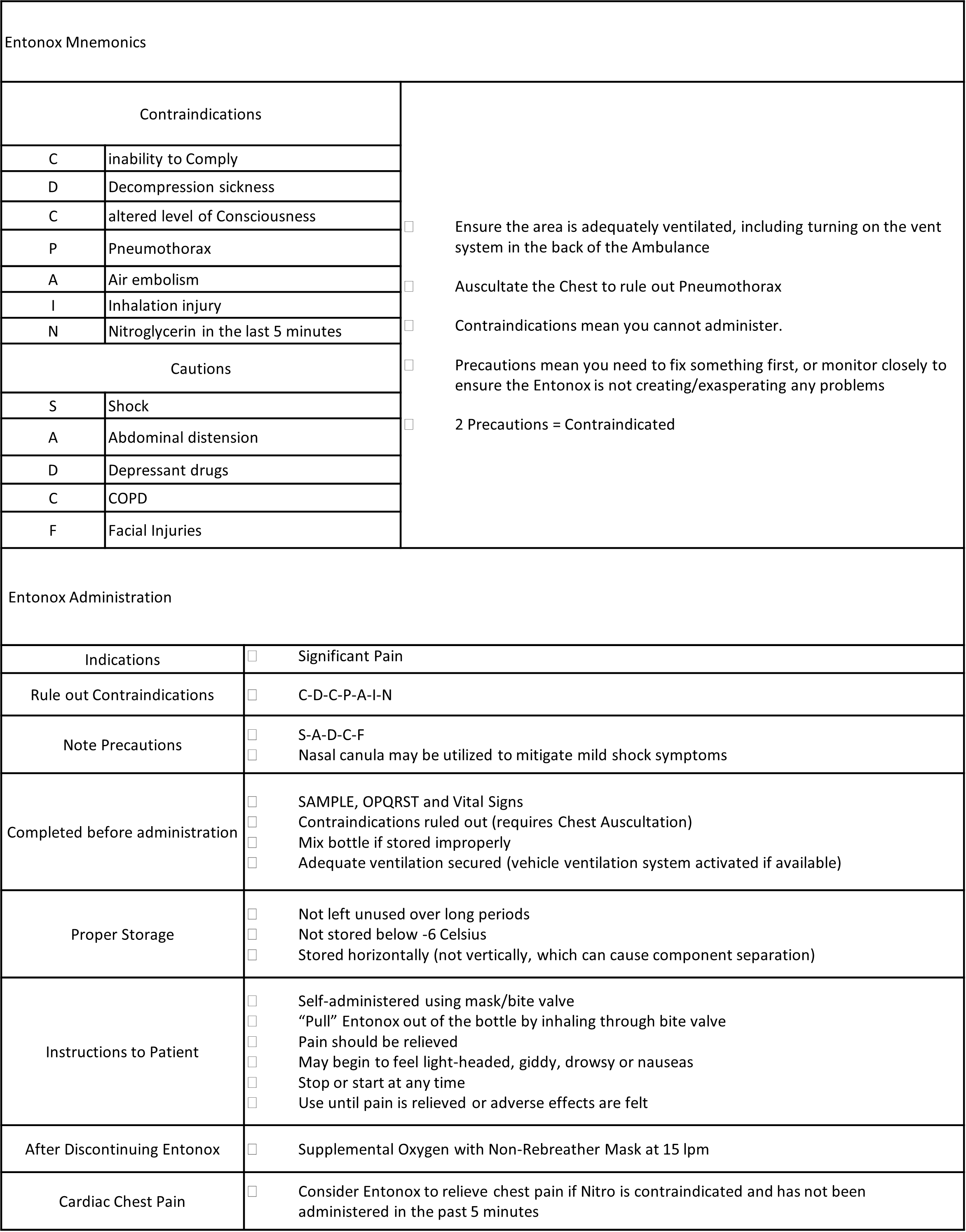
Nitrous Oxide (Entonox), also commonly referred to as laughing gas, is a fast acting analgesic gas which can be self-administered by patients under the guideance and supervision of a Licensed Emergency Medical Responder in BC. Entonox is indicated, and should be considered, for any patient experiencing significant pain or physical discomfort, however the corresponding gases that permeate the lungs and bloodstream can cause significantly negative patient outcomes if contraindicated. Most often, Entonox is provided to patients with a simple, non-life-threatening femur fracture as part of applying a Sager Traction Splint. Entonox is also appropriate for patients experiencing cardiac chest pains if Nitroglycerin is contraindicated or not available.
What the EMALB Examination Guidelines say:
Entonox Indications
Entonox Contraindications
Entonox Cautions
Entonox Protocol
What this means for Emergency Medical Responders in BC:
Administration of Naloxone (Narcan) to Reverse Opioid Overdose
.jpg "Emergency Medical Assistants Licensing Board British Columbia Provincial EMR Examination Guidelines for Administration of Naloxone (Narcan) to a patient experiencing significant pain or discomfort.")
Administering Narcan, in either intramuscular or intrnasal form can temporarily alleviate the most life-threatening aspects of Opioid overdose, such as respiratory arrest and unresponsiveness, but it does not completely remove the poison from the person's system. The opioids will remain in the system after the Naloxone has dissipated, so it is vital that someone receives definitive clinical medical care as soon as possible following the overdose and subsequent Narcan administration. The administration of Naloxone, once appropriate, may further support these critical interventions by increasing the patient's level of conciousness and/or improving their natural respiration rate, rhythm and character. Although multiple doses of Naloxone, at increasing dosages, may be required for optimal patient care, it is not necessary to completely reverse all the effects of the opoiod or achieve full patient responsiveness, as long as the airway remains clear and adequate respirations resume.
What the EMALB Examination Guidelines say:
Naloxone (Narcan) is a narcotic antagonist which antagonizes opioid effects by competing for the same receptor sites. This antagonistic action reverses the effects of opioids including respiratory depression, sedation, and hypotension.
Naloxone Indications
Naloxone Contraindications
Naloxone Cautions
Prior to Naloxone Administration
First Naloxone Dose
Second Naloxone Dose
Third Naloxone Dose
Fourth Naloxone Dose
Contradictory information in the BC Emergency Health Services Act:
What this means for Emergency Medical Responders in BC:
Examination Guidelines Contents:
EMA Licensing Board Examinations
EMA Licensing Board Examination Policies